- Joined
- Jun 16, 2021
- Messages
- 2,366
- Reaction score
- 2,605
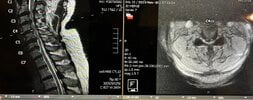
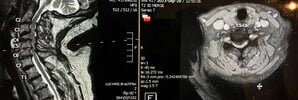
Cervical block vertebrae as well.

View attachment 379265View attachment 379266
Start with a couple epidermals, then catterize them nerves.
Anyone want to see this patient, pretty sure I cannot help.
Axials don’t look bad. I’d inject that all dayThis'll go great for all of us...
View attachment 379328View attachment 379332View attachment 379329View attachment 379330View attachment 379331
I think they look quite bad.Axials don’t look bad
Young grasshopperI think they look quite bad.
After how many pts does one become seasoned enough to comment? Of course I'd inject this, and if this lady shows up on time and doesn't cuss out my phone service I'll probably offer her procedural based pain management but look at all that fat.Young grasshopper
She will not. L2-S1 fusion will make her worse.After how many pts does one become seasoned enough to comment? Of course I'd inject this, and if this lady shows up on time and doesn't cuss out my phone service I'll probably offer her procedural based pain management but look at all that fat.
She won't get better with anything I do.
Entire point of my post.She will not. L2-S1 fusion will make her worse.
RFA, ESI will fail. SCS will get her 1 year of relief then fail.
Mounjaro might be best injection for this patient.
Ahhh I misunderstood your post. I thought you were concerned about the degree of stenosis. My eyes went straight to the spine. I didn’t even look at all her back fat. This is where seeing the patient and the entire clinical picture helpsAfter how many pts does one become seasoned enough to comment? Of course I'd inject this, and if this lady shows up on time and doesn't cuss out my phone service I'll probably offer her procedural based pain management but look at all that fat.
She won't get better with anything I do.
i guess you dont see these patients often enough...Entire point of my post.
No potential for salvage.
Multilevel disk collapse with pan lumbar stenosis. She's 5'3" and 300 lbs (taxes ought not to pay for your bag of fudge rounds)...
I'll listen to her and give her the 3 min she wants to vent about her shortcomings in life, then I'll offer a few shots and in the end nothing will change and she will not benefit from seeing me.
She called 20 min late today and was en route. Yelled at my call service. I refused to see her.
We rescheduled her and she has one more chance or she's fired.
Scoliosis is minimal despite the way it appears on that saggital view. If she shows up on time I'll see her. I refused to see her Friday bc she was way too late AND was rude to our phone ppl.i guess you dont see these patients often enough...
this is like 20% of my patient population.
fwiw, she has some degree of scoliosis, so the stenosis is probably not as bad as visualized on the one sagittal.
how you can help make her better -
1. try one epidural. use a 7 inch needle. i have a bunch in stock, if you need them.
2. discuss weight loss
3. refer her to bariatrics. even if she loses 20 pounds with mounjaro, she wont get markedly better.
4. tell her that she can make changes if she chooses to, but it is hard work. she is the one that can make herself better.
This one's brutal...That's the best axial I can do.
Hx breast cancer. Severe back and leg pain.
View attachment 379433
View attachment 379434
View attachment 379435
View attachment 379436
C2-6 ACDF vs ACDF then Posterior cleanup. For both.Here are two doozies. One patient better with PT and refusing to see the surgeon. Other patient can barely walk and previous doc chalked it up to issue prior to lumbar lami. Fortunately got her in with another surgeon who’s gonna operate
View attachment 379265View attachment 379266
Start with a couple epidermals, then catterize them nerves.
Anyone want to see this patient, pretty sure I cannot help.
I vote auto-fusion because of the halo of bone around the fused level, and the myelomalacia in an area where there’s still CSF around the cord, which suggests to me the process may have started with a high-energy impact at some point in the distant past, causing cord damage and trashing the disc.Klippel-Feil or complete disk collapse?
View attachment 379602View attachment 379606View attachment 379605View attachment 379604
What's going on with the intensity in the spinous process?Klippel-Feil or complete disk collapse?
View attachment 379602View attachment 379606View attachment 379605View attachment 379604
Maybe stress reaction? She's got cervical scoli and listhesis at multiple levels, notably that same level. Here's an axial right there:What's going on with the intensity in the spinous process?
This is weird. It is unusual to get a wet tap this far lateral. Dural sleeve must have been unusually long.View attachment 379081
Another linkedin hero. He knew he was not epidural. But he did not know he was IT.
Retracted the needleThis is weird. It is unusual to get a wet tap this far lateral. Dural sleeve must have been unusually long.
Not squared AP, might be more medial than appearsThis is weird. It is unusual to get a wet tap this far lateral. Dural sleeve must have been unusually long.
All from same doc? In Athens?
Opiate refugee.All from same doc? In Athens?
SO how did the MBBs go?View attachment 380247
This was a bummer, sent for back pain and referral to try mbb. Had seen surgeon who was hoping RFA would help. Known Cancer, no mets to spine. He mentioned new leg length discrepancy.........
Jewett style brace. Tymlos. Wouldn't mind kypho of lower Fx, but it looks like T4 and T6 are the new ones. If local guy would do spine jack at T4, he can have both Fxs to fix.
Unnecessary fusion again. Normal disc. No listhesis. L3 screw is subpedicular.View attachment 380596
Nails on chalkboard
(Season 1 Jack Ryan and apparently he has the spine of a 55 yo female)
Well, the apparent fusion is at L3-L4, not L4-L5.View attachment 380596
Nails on chalkboard
(Season 1 Jack Ryan and apparently he has the spine of a 55 yo female)
Did the uppers not get reported to the pdmp?
Interesting. Not sure that's not a facet cyst. Looks like a small one coming off the right posterior facet. Never seen a disc cystSaw this today. 27 yr old man. Does manual labor. Has left L5 radicular pain.
MRI report states they think the cyst arises from the disc.
My first step is clear, a left L4-L5, L5-S1 TFESI. The next step is less clear. I had a mental debate about trying the rupture the cyst with a transforaminal approach and using discogram protocosl (IV abx and double needle) .
Or I could send him straight surgery if he fails the TFESI, I suppose.
View attachment 381214
View attachment 381215
I’d try the TFESI then send to surgery. Not worth trying to be a hero over, especially for something they can probably deal with permanently through a 1” incision. Have never heard of a disc cyst. Perineal cyst maybe.Saw this today. 27 yr old man. Does manual labor. Has left L5 radicular pain.
MRI report states they think the cyst arises from the disc.
My first step is clear, a left L4-L5, L5-S1 TFESI. The next step is less clear. I had a mental debate about trying the rupture the cyst with a transforaminal approach and using discogram protocosl (IV abx and double needle) .
Or I could send him straight surgery if he fails the TFESI, I suppose.
View attachment 381214
View attachment 381215
I’d do this, too. Would be interested if contrast in facet showed this filling.i have seen disc cysts. but they are much smaller.
you could try to aspirate the cyst via a facet approach -- as it is most likely a facet cyst. but, that may not get paid, and you would have to do it on a separate visit from the TFESI.
i like to do a TFESI AND facet aspiration/injection at the same time but that is getting harder and harder to get covered.