the quote should be "better teach this kid some control before he kills somebody"Juuuust a bit outside

could apply to the surgeon as well.....

the quote should be "better teach this kid some control before he kills somebody"Juuuust a bit outside
Bet she gets 3+ months. Depo for the win again. It just works betterNice patient with small but painful central-paramedian thoracic disc, and thoracic radiculopathy. Failed conservative care.
Did an TESI with depo but did nothing as her disc is almost midline and a thoracic ILESI will not spread that far ventral . Then I did a thoracic TFESI with dex, which gave her 90% relief for 6 days and then all her pain returned.
So today, I did a TESI with cath and as you can see I essentially gave her a thoracic TFESI but with depomedrol. There is excellent spread along her thoracic nerve root and excellent thoracic anterior epidural spread of depomedrol! I'm looking forward to her next follow-up.
View attachment 377287
View attachment 377288
Yeah, i see it. Sturdy hinged brace for transfers. Should heal, actually95 yo F on chronic Norco 7.5 BID. Back is terrible. Actually was run over by a car in a scooter at a grocery store a year ago. Maybe 3-4 weeks ago fell and landed on her left knee.
She never stands up anyways other than to transfer. She can transfer on this knee. I recommended a basic support brace and we're leaving it alone.
Pretty sure she's got a tibial plateau fracture.
View attachment 377639View attachment 377640View attachment 377641
Meet the D of the Week:40 yo Hispanic M in an MVC with an MRI report that reads multi level HNP. No stenosis of course.
An outside NP did bilateral C5-7 MBB with PRP x 2. These failed of course. Interestingly, they originally scheduled for PRP in the elbow (the wreck caused epicondylitis apparently), but the pt showed up and got an MBB at C5-7 with the PRP. They then offered an ESI which never took place, and then surgery.
Yall want yalls mom getting bilateral C5-7 MBB with PRP? Which PRP you may ask? Leukocyte poor? Rich? I don't F'ing know...Prob the NP didn't either!
Gets better - The NP who did it...On LinkedIn he completed an American Academy of Procedural Medicine course in Jan '23. I go to the AAOPM page. Ever seen that BS? There are 1-3 days courses for a few thousand each.
Hilarious - The MD who did the first PRP MB "block" is a medical director and claims reviewer for an insurance company. So, he's doing absurd BS in his clinic while preventing others from getting MRIs and doing visco and ****...
View attachment 377768
View attachment 377769

 www.gaspine-ortho.com
www.gaspine-ortho.com
Not the same group. It's super confusing.
Needs some explanation.Not the same group. It's super confusing.
There's another group by the same name. Larger group. It's like 3-4 surgeons, a neurologist and a PMR guy.Needs some explanation.
what species is that?
Easy one. Put in a pair of 16G RF needles and hook up to some jumper cables.
Intracept at L3-4 then SCS at T12-L1 (I see you lamina of L1)
Atraumatic and deadlifting don't go together until your form is perfect, and even then it seems like a bad idea.34 year old, 4 years atraumatic low back pain with some right L5 distribution radicular pain that began after doing some deadlifts. No other trauma or surgical history.

 www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
give the guy a break. he's got other things to worry about right now. check out the proximity.....View attachment 378294View attachment 378295View attachment 378296
LinkedIn Login, Sign in | LinkedIn
Login to LinkedIn to keep in touch with people you know, share ideas, and build your career.www.linkedin.com

Fascinating. I've never seen a laminar fracture like this before -- usually I think about them as high impact trauma injuries. That article does give some insight though.Atraumatic and deadlifting don't go together until your form is perfect, and even then it seems like a bad idea.
"While performing 75 to 100% of individual 1RM, maximum compressive spinal forces can reach 18 kN among men and 8 kN among women, and maximum shearing spinal forces can reach 3 kN among men and 2 kN among women. These values are concerning given reported injury thresholds for the lumbar spine segments that range between 5 – 10 kN and 1 – 2 kN, for compressive and shearing forces, respectively."Low Back Biomechanics during Repetitive Deadlifts: A Narrative Review
Low back pain is a significant problem and one of the primary musculoskeletal conditions affecting active duty service members. There is a need to comprehensively assess the effects of repetitive deadlifts as a physical training modality on lumbar spine ...
Ego lifting is dangerous. See 1-2 per week of bro-science lifters with acute discs.Atraumatic and deadlifting don't go together until your form is perfect, and even then it seems like a bad idea.
"While performing 75 to 100% of individual 1RM, maximum compressive spinal forces can reach 18 kN among men and 8 kN among women, and maximum shearing spinal forces can reach 3 kN among men and 2 kN among women. These values are concerning given reported injury thresholds for the lumbar spine segments that range between 5 – 10 kN and 1 – 2 kN, for compressive and shearing forces, respectively."Low Back Biomechanics during Repetitive Deadlifts: A Narrative Review
Low back pain is a significant problem and one of the primary musculoskeletal conditions affecting active duty service members. There is a need to comprehensively assess the effects of repetitive deadlifts as a physical training modality on lumbar spine ...
Jeez! How common is it for NPs to do spine procedures much less cervical epidurals?40 yo Hispanic M in an MVC with an MRI report that reads multi level HNP. No stenosis of course.
An outside NP did bilateral C5-7 MBB with PRP x 2. These failed of course. Interestingly, they originally scheduled for PRP in the elbow (the wreck caused epicondylitis apparently), but the pt showed up and got an MBB at C5-7 with the PRP. They then offered an ESI which never took place, and then surgery.
Yall want yalls mom getting bilateral C5-7 MBB with PRP? Which PRP you may ask? Leukocyte poor? Rich? I don't F'ing know...Prob the NP didn't either!
Gets better - The NP who did it...On LinkedIn he completed an American Academy of Procedural Medicine course in Jan '23. I go to the AAOPM page. Ever seen that BS? There are 1-3 days courses for a few thousand each.
Hilarious - The MD who did the first PRP MB "block" is a medical director and claims reviewer for an insurance company. So, he's doing absurd BS in his clinic while preventing others from getting MRIs and doing visco and ****...
View attachment 377768
View attachment 377769
Pretty common. When I was interviewing for PAs a yr or two ago I had a 4'10" PA I spoke with who was the sole proceduralist for a neurosurgery group. I told him that's not gonna happen in our practice. He wanted to do stimulators and everything. Haha...Never gonna happen bro.Jeez! How common is it for NPs to do spine procedures much less cervical epidurals?
Bourbon in a Islay barrel sounds like an abomination. Is it any good? I picked up some Old Forrester 1920 and have really been enjoying it.Pretty common. When I was interviewing for PAs a yr or two ago I had a 4'10" PA I spoke with who was the sole proceduralist for a neurosurgery group. I told him that's not gonna happen in our practice. He wanted to do stimulators and everything. Haha...Never gonna happen bro.
Speaking of pictures...Georgia vs Florida today. World's Largest Outdoor Cocktail Party.
Abomination? Live life bro...Try stuff...Appreciate creativity. No reason to think anything negative about Bourbon in a scotch barrel.Bourbon in a Islay barrel sounds like an abomination. Is it any good? I picked up some Old Forrester 1920 and have really been enjoying it.
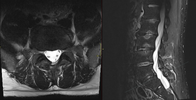
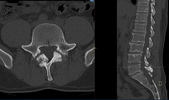
Are we thinking we are looking at leptomeningeal disease/drop mets?70-75 y/o man with Clbp. Had RFA 3 years ago with good results. Repeated a month ago. No relief. Pain worse, MRI prior to interventional care with DDD, mod foraminal stenosis and worsening leg pain. Better in flexion. ESI relief x1 day. Calls back and pain worse. Demands to be seen. Get ESR/CRP/CBC. MRI repeat with contrast. Labs normal. Contrast views above. None of this seen less than 2 months ago on non contrast MRI. Neurology consulted. Neurosurgery consulted. Broad differential diagnosis. None of it good or that we treat. Going to get liberal with meds.
No. We ARE looking at that.Are we thinking we are looking at leptomeningeal disease/drop mets?
What's the non-con MRI FS sequence show prior to your intervention? No hint of disease in retrospect?No. We ARE looking at that.
Nothing there. Just arthropathy.What's the non-con MRI FS sequence show prior to your intervention? No hint of disease in retrospect?
LMD sucks to treat and would plug in with palliative for GOC discussion if you're not running point on that. Palliative radiation/chemo could buy time if no prior cancer tx, but I assume his primary is something that was treated remotely.
Least fav procedure. I find facet injxns very difficult.Facet cyst aspiration. It always makes me happy when something actually comes out!
have to look at the MRI cuts. it is a difficult injection when the facets are hypertrophic you ssmetimes have to come in AP or even contralateral oblique. the osteophytes can wrap around the joint making it really difficult to get in.
but that it legit joint fluid
do you have this?There’s a great case discussion on SIS where Tim Maus shows how to do these using CLO approach to rupture cysts when there is a lot of SAP hypertrophy. Has improved my success rate of getting access to these joints drastically.
It’s just gonna come back. They suck but nice dopamine hit for a bitFacet cyst aspiration. It always makes me happy when something actually comes out!
Aren’t intra-articular facets considered all sham all the time now? Mbb for all according to all payorsLeast fav procedure. I find facet injxns very difficult.
I have a handful of <50 age patients with mild OA or random facet effusion that get approved and do well ... but yes almost all are MBB/RF.Aren’t intra-articular facets considered all sham all the time now? Mbb for all according to all payors