I'd say that's a bold interpretation of the trial. Showed no statistically significant difference in any of the mentioned end points between T and placebo. While VTEs were 1.7% in T arm vs. 1.2% in placebo arm, you could just as easily point to death from CV causes at 3.4% in T arm and 4.0% in placebo arm. Neither are significant.
We can make plenty of statements about safety of T and prostate cancer
"There is no clinical evidence that testosterone therapy increases risk of recurrence or progression of prostate cancer"
In men with prostate cancer, there is no risk that higher endogenous testosterone levels increases risk of recurrence or progression (except when on ADT)
"There is retrospective evidence that testosterone therapy does not increase risk of recurrence or progression of prostate cancer"
The safety of testosterone therapy (TT) after definitive treatment for localized prostate cancer remains undefined. We analyzed the risks of biochemical recurrence and mortality in men receiving TT after treatment for localized prostate cancer. Cohort analysis using the national US Veterans...

www.nature.com
"patients without prostate cancer on testosterone therapy do not have a higher risk of developing prostate cancer"
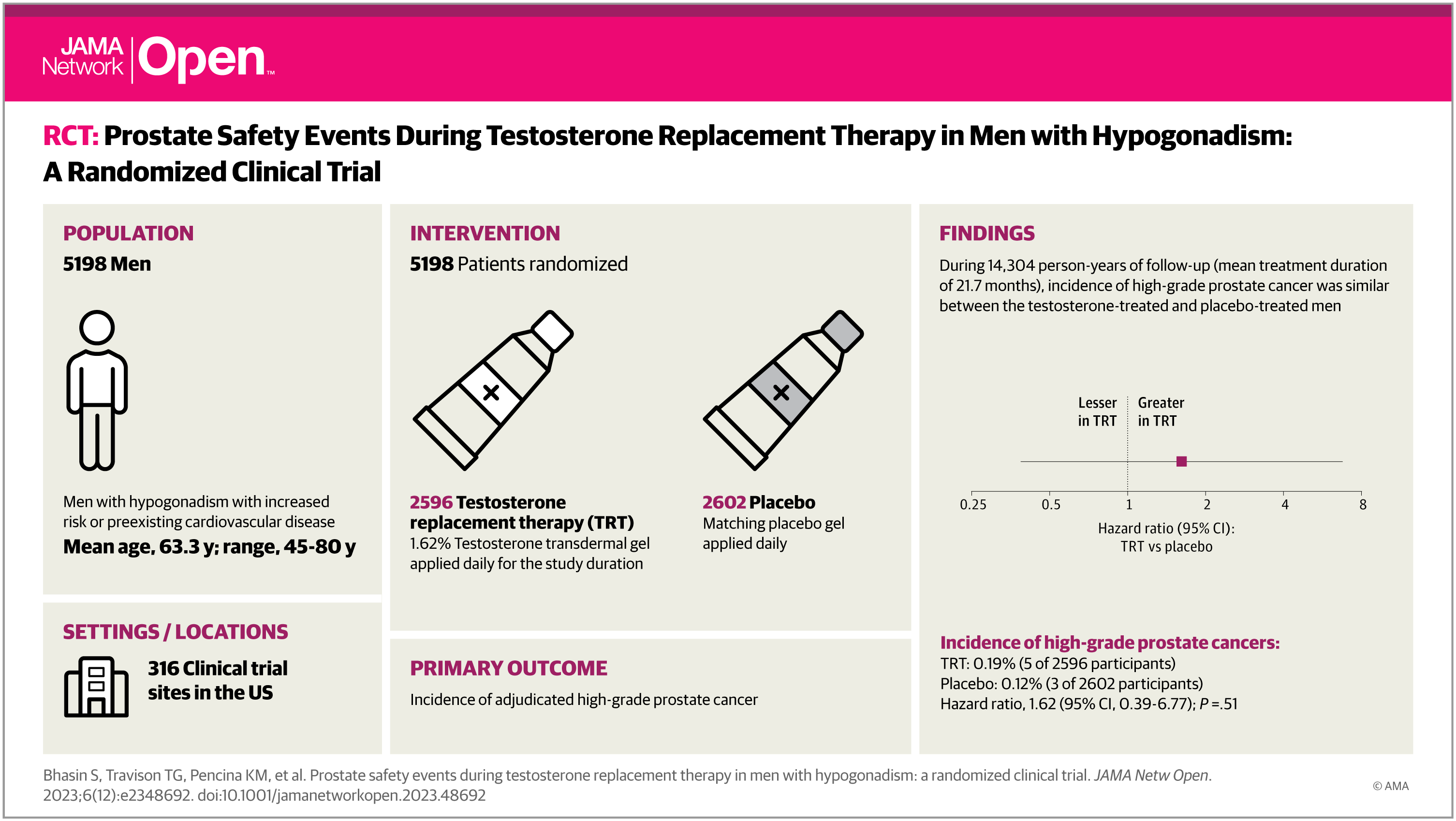
This randomized clinical trial examines the effects of testosterone replacement therapy on major adverse cardiovascular events in men with hypogonadism.

jamanetwork.com
The whole T and prostate cancer story to me is an interesting one. We create these stories in our heads that have no basis in scientific fact, such as "we lower T to treat prostate cancer, thus higher T must be bad for prostate cancer", and then it becomes incumbent on us to create mountains of evidence to overcome the supposition that is based on an idea with no evidence. All the while ignoring the fact that men naturally produce testosterone, and except when trying to reach castrate levels we do nothing to modulate it (for good reason) in the management of prostate cancer.
We also have no data about the effects of ozempic on prostate cancer recurrence, and yet we are happy to give it.