
- Joined
- Feb 1, 2005
- Messages
- 4,927
- Reaction score
- 1,913
I would love to see the citation on that. I’d bet it’s empirical.View attachment 365162
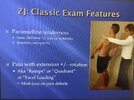
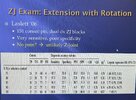
This is a snippet from Benzon, written by Steve Cohen. The best and only reliable PE maneuver is paraspinal tenderness. I am happy to see other literature supporting other PE maneuvers. Can we even claim that extension best exacerbates the most commonly implicated joints of 4-5 and 5-1?
This is from a lecture I put together as a fellow and one I give to residents every year.
Attachments
-
 40932853-237A-4251-8A4E-6D87324FDDB7.jpeg259 KB · Views: 107
40932853-237A-4251-8A4E-6D87324FDDB7.jpeg259 KB · Views: 107 -
 46376FA6-4FB6-4A4B-891F-20796078CA59.jpeg272.2 KB · Views: 101
46376FA6-4FB6-4A4B-891F-20796078CA59.jpeg272.2 KB · Views: 101 -
 D0C2650D-921E-4EE4-A5CE-7C02E5807605.jpeg201.6 KB · Views: 99
D0C2650D-921E-4EE4-A5CE-7C02E5807605.jpeg201.6 KB · Views: 99 -
 A1D4A6F0-3021-43E5-8FD8-188944B1C541.jpeg243.5 KB · Views: 111
A1D4A6F0-3021-43E5-8FD8-188944B1C541.jpeg243.5 KB · Views: 111 -
 5F77ADF1-97C7-4F21-A38A-B1ECA59CD5A2.jpeg268.5 KB · Views: 99
5F77ADF1-97C7-4F21-A38A-B1ECA59CD5A2.jpeg268.5 KB · Views: 99


")